
Yes, this is a structural biomechanical model. I am fully aware of the pain science and biopsychosocial concerns we employ in the clinic. But this essay here is purely to common pathomechanics concerns.
One cannot reasonably generalize, of course, about low back problems. …BUT… the onset of workplace Low Back Pain-Injury often follows a common “cascade of dysfunctions” that may help to define a course of mgt (prevention & recovery).
Let us describe a typical course of evolving dysfunction, leading to degeneration, leading to derangement… typical pathomechanics… which can then define a list of targets for the PT to pursue in primary prevention as well as treatment, recovery, return to work.
This is the story I tell workers in the course of our prevention program… and what I tell patients seeking recovery. Important… the only P.T. intervention that is truly effective on the long-term is: education (patient education and worker education) to make the individual an EXPERT on how their low back is put together mechanically, how it works mechanically, how it breaks down mechanically. This informs, empowers, and motivates the individual to take control of their risk factors and spinal mechanics… and achieve effective recovery and prevention. And, again, we must also consider the biopsychosocial model.
The story… Part 1… The vertebra bones sit on one another, weight shared between the discs and facet joints (show them the picture of this). The disc is 80% water (when you are 20 yrs old)… but gradually loses that water over time, dropping to 40% water around 40 yrs old. Disc goes from 2/3 inch thick to 1/3 inch thick. This is a degenerated disc. That increases weight on facet joints by 200-300%. That can lead to degenerative joint changes. Pain-stiffness leads to muscle weakness, reducing muscle control, allowing strain-sprain-instability.
Part 2… How I explain it to worker or patient: We spend so much of life sitting and bending. This shifts weight from facet joints to disc, especially the back half of the disc. This speeds the out-flow of water from disc. It also shifts-leans the nucleus of the disc posteriorly against the back wall of disc. Sitting and bending over-stretches that back wall. Back wall of disc eventually weakens and over stretches, allowing jelly center to push out on wall… bulging disc. Wall can eventually fail to contain the jelly, and it blows through… herniated disc. NOTE… this does not cause pain (very few pain nerves in the disc itself)… unless the bulge or herniation pushes on other structures that are pain-sensitive.
Part 3… Shrinkage of disc or herniation-bulge reduces the space between vertebae. That allows ligaments that support and stabilize the spine to go slack. Bones now unstable, shifting abnormally during movement, causing sprain, strain, damage, apin.
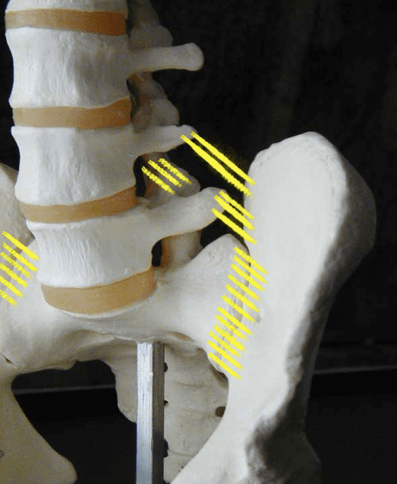
Part 4… This instability is especially an issue where pelvis bone attaches to spine (sacro-iliac joint). This is very stable joint that hardly moves at all, held snug by ligaments. Some of those ligaments come off the lower two vertebrae (L4 or L5) (iliolumbar ligaments). If there is reduced or bulging discs at L4-L5-S1, then iliolumbar ligaments go slightly slack, causing abnormal stress-strain at sacroliac joint. This can cause Rotator Cuff of hip (piriformis) to tighten as it tries to help support the sacroiliac joint. This causes that pain-spasm deep in the buttock. Piriformis pulls on its tendon at hip, leading to hip bursitis. It also compresses hip risking hip arthritis. Thight piriformis can also compress sciatic nerve running underneath it… one more cause of sciatica.
The story… changes at disc, allow ligaments to no longer adequately support sacoiliac, causing tight piriformis, irritating hip and sciatic nerve.
Treatment sequence typically calls for restoring disc mechanics (usually with lower back extension stretches)… stretching hamstrings that may be pulling abnormally on pelvis to stress sacroiliac… stretching muscles at front and back of hip (single knee-to chest with other leg totally flat) to reduce sacroiliac stress and strain… stretching piriformis to reduce its stress and strain to sacroiliac-sciatic-hip.
Then, once disc mechanics and muscle flexibility stresses are improved, we must strengthen the deepest layers of spine stability muscles… supine powerbridges, prone planks, side planks, and quadrupedal multifidus.
Yes, we are threatening to attempt proposing a general low back care protocol with this essay… but it is a good basis for address the pathomechanics of a large group of workplace low back “injuries” and aging worker concerns.
disc mechanics affects facet WB and lig support, which affects SIJ support, affected by hams & piriformis function.
I will add link here to a powerpoint/PDF of the seminar I teach on this topic… at…
LB-Rx
Low Back Dysfunction eBook: LOW.BACK
