My favorite PT motto is “Be An Inch Taller” !
FHP, round-shoulders, slouching… This is the basis for so much aging effects as well as workplace ergonomics and MSD risks.
Think about it… how many UE MSD issues such as longstanding tendinitis-tendinosis, plus neurovascular entrapments such as CTS, cubital tunnel syndrome (underling so many golfers elbow, med epicond), pronator NVE, radial tunnel (underlying so many tennis elbow, lat epi), and other overuse sx… how many actually have potential inputs from some degree of thoracic outlet-inlet compression?? How many have neurogenic nociceptive effects from cervical-thoracic posture strain?? Many? Most??
FHP is almost always present with sustained sitting and prolonged standing. Gravity wins. Worsens with fatigue.
FHP: Fixed flexion of upper thoracic (sustained tension of post ligaments of upper thoracic blanching their blood supply, creating ischemic pain, with nearby secondary spasm) (abnormal loads on discs and facet joints, speeding degeneration). This also creates a stretch weakness of thoracic and scapular stabilizers
FHP: With flexed upper thoracic, there will be hyperextension at upper cervical to restore level vision. This compresses subcranial tissues, including greater occipital neurovascular bundle.. headache), as well as upper cervical facets in a close-packed position (DJD). This also creates the flattening of mid-cervical lordosis. This degenerates those discs, bringing the uncus of the vertbrae together to form an unco-vertebral joint (joint of vonLusca) leading to the infamous bone spurring at C5-6!
FHP: lateral neck muscles responsible for keeping vision level-horizontal (scaleni) must now shorten to do their job, compressing brachial plexus and obstructing venous-lymph flow out of the UE… backup of interstitial fluids down the UE… slight compression of nerves, causing swelling and irritation further down the arm… TOC leading to double-crush at various “tunnels” in UE.
FHP: tilts shoulder blade to compress the space occupied by the rotator cuff, reducing blood supply and compressing tissues.
FHP: in standing, there will be a compensatory flattening of the lumbar to maintain balance. This risks degenerated, bulging, herniated lumbar discs.
FHP: Pulls on infra-hyoid muscles of swallowing, pulling down on jaw, which is countered by excessive posture work from massetter muscle trying to keep mouth closed. Leads to over-closing jaw, causing TMJ problems (my favorite patient challenge, so easy to improve).
FHP: Compresses lungs down into diaphragm, flattening it, reducing its breathing role, shifting breathing to scaleni for paradoxical breathing that shortens and overloads scaleni (more TOC risk).
PREVENTION: Be An Inch Taller! and people will comply once properly educated on this, a simple self-awareness that may improve posture by 10% about 10% of the time… often enough to reverse or at least slow the damage. Frequent micro-stretches (10 sec) at scalenus medius-anticus, and axial-extended chin-tucks. Frequently switch between sitting and standing, such as using the Vari-Desk on computer jobs. Strengthen upper back (Theraband scap retract, eg). Lateral pterygoid exercises to quiet and correct TMJ.
FHP looking down by flex neck on thoracic 
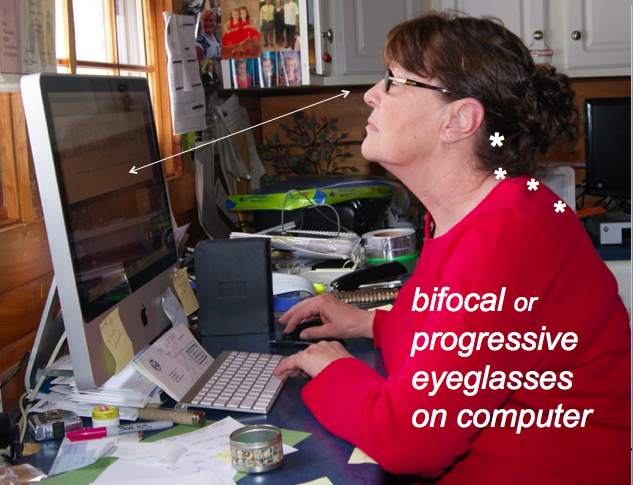
Bifocals while working on computer…